Simulaite Report
Berberine Bioavailability — 5-Arm Formulation Comparison
Capsule vs Piperine Co-Administration vs Mucoadhesive Buccal Strip
April 26, 2026
Executive Summary
We simulated oral bioavailability (F) for berberine across five delivery arms — capsule 500mg (fed and fasted), capsule 500mg co-administered with piperine 4.75mg (fasted), and a mucoadhesive buccal strip 40mg (standard and ideal patient, fasted) — using the Simulaite PBPK engine on a virtual population of 100 American individuals
(age 30–65). Berberine has surged in popularity as a natural GLP-1 pathway activator and metabolic health ingredient, yet it remains a permanently charged quaternary alkaloid with notoriously poor oral bioavailability. This simulation maps the mechanistic reasons why different enhancement strategies succeed or fail.
- Baseline capsule F is 0.30% (fasted) — food has zero effect (0.30% fed), confirming berberine's permanent charge blocks lipid-mediated solubilization
- Piperine co-administration raises F to 0.83% — a 2.8× boost — by blocking gut-wall and liver CYP enzymes and P-gp efflux pumps
- Buccal strip (ideal patient) achieves 1.36% F but delivers only 0.54 mg-equiv absolute exposure vs 1.50 mg-equiv for the plain capsule — the dose constraint defeats the route advantage
- Berberine's permanent charge (quaternary N+) locks it out of transcellular buccal absorption — paracellular-only transport through tight junctions limits mucosal permeability regardless of formulation
- Practical recommendation: piperine co-administration or switching to dihydroberberine (uncharged analog, better absorption shown in clinical literature) are more effective than reformulating the delivery route
Key Takeaways
Simulation Inputs
Molecules
| Name | SMILES | MW (g/mol) |
|---|---|---|
| Berberine | COC1=C(C2=C[N+]3=C(C=C2C=C1)C4=CC5=C(C=C4CC3)OCO5)OC | 336.367 |
| Piperine (co-admin) | C1CCN(CC1)C(=O)/C=C/C=C/C2=CC3=C(C=C2)OCO3 | 285.343 |
Berberine is a quaternary ammonium alkaloid with a permanent positive charge at all physiological pH values. Its permanent charge is the dominant barrier to both oral and buccal absorption. Piperine is a bioenhancer alkaloid from black pepper that inhibits gutwall and liver CYP enzymes and P-gp efflux pumps, increasing berberine bioavailability when co-administered.
Formulation Parameters
1. Capsule 500mg — Fed
- Delivery Type
- Oral capsule
- Route
- Oral (swallowed)
- Dose
- 500 mg berberine
- Prandial State
- Fed (with meal)
- Particle Size
- Mean radius 25µm, SD 10µm
2. Capsule 500mg — Fasted
- Delivery Type
- Oral capsule
- Route
- Oral (swallowed)
- Dose
- 500 mg berberine
- Prandial State
- Fasted
- Particle Size
- Mean radius 25µm, SD 10µm
3. Capsule 500mg + Piperine 4.75mg — Fasted
- Delivery Type
- Oral capsule
- Route
- Oral (swallowed)
- Dose
- 500 mg berberine + 4.75 mg piperine
- Prandial State
- Fasted
4. Buccal Strip 40mg — Standard Patient
- Delivery Type
- Mucoadhesive buccal strip
- Route
- Buccal (cheek)
- Surface Area
- 3 × 4 cm (12 cm²)
- Dose
- 40 mg berberine
- Prandial State
- Fasted
- Patient Type
- Standard (includes natural swallowing)
5. Buccal Strip 40mg — Ideal Patient
- Delivery Type
- Mucoadhesive buccal strip
- Route
- Buccal (cheek)
- Surface Area
- 3 × 4 cm (12 cm²)
- Dose
- 40 mg berberine
- Prandial State
- Fasted
- Patient Type
- Ideal (refrains from swallowing during dissolution)
Population Settings
| Parameter | Value |
|---|---|
| Sample Size (n) | 100 |
| Sex | 49% female, 51% male |
| Age Range | 30.4–64.5 years (mean 45.9) |
| Body Weight | 47.9–146.2 kg (mean 80.8) |
| BMI Range | 18.2–62.6 (mean 28.4) |
| Ethnicity | White 62% · Latino 19% · African American 13% · Asian 6% |
| Prandial State | Fasted (capsule arms); Fed (capsule fed arm) |
Bioavailability Results
PK Parameters — All Arms
| Arm | F% (mean±SD) | CV% | Cmax (µmol/L) | Tmax (h) | Abs. Exposure |
|---|---|---|---|---|---|
| Capsule 500mg — Fed | 0.30 ± 0.19% | 63% | 0.2117 | 0.6 | 1.50 mg-equiv |
| Capsule 500mg — Fasted | 0.30 ± 0.19% | 63% | 0.2117 | 0.6 | 1.50 mg-equiv |
| Capsule 500mg + Piperine 4.75mg — Fasted | 0.83 ± 0.51% | 61% | 0.5835 | 0.6 | 4.15 mg-equiv |
| Buccal Strip 40mg — Standard Patient | 0.65 ± 0.19% | 29% | 0.0116 | 2.0 | 0.26 mg-equiv |
| Buccal Strip 40mg — Ideal Patient | 1.36 ± 0.21% | 15% | 0.0152 | 13.0 | 0.54 mg-equiv |
Abs. Exposure = F% × dose — the actual mg of berberine reaching systemic circulation. This is the clinically relevant metric when comparing arms with different doses.
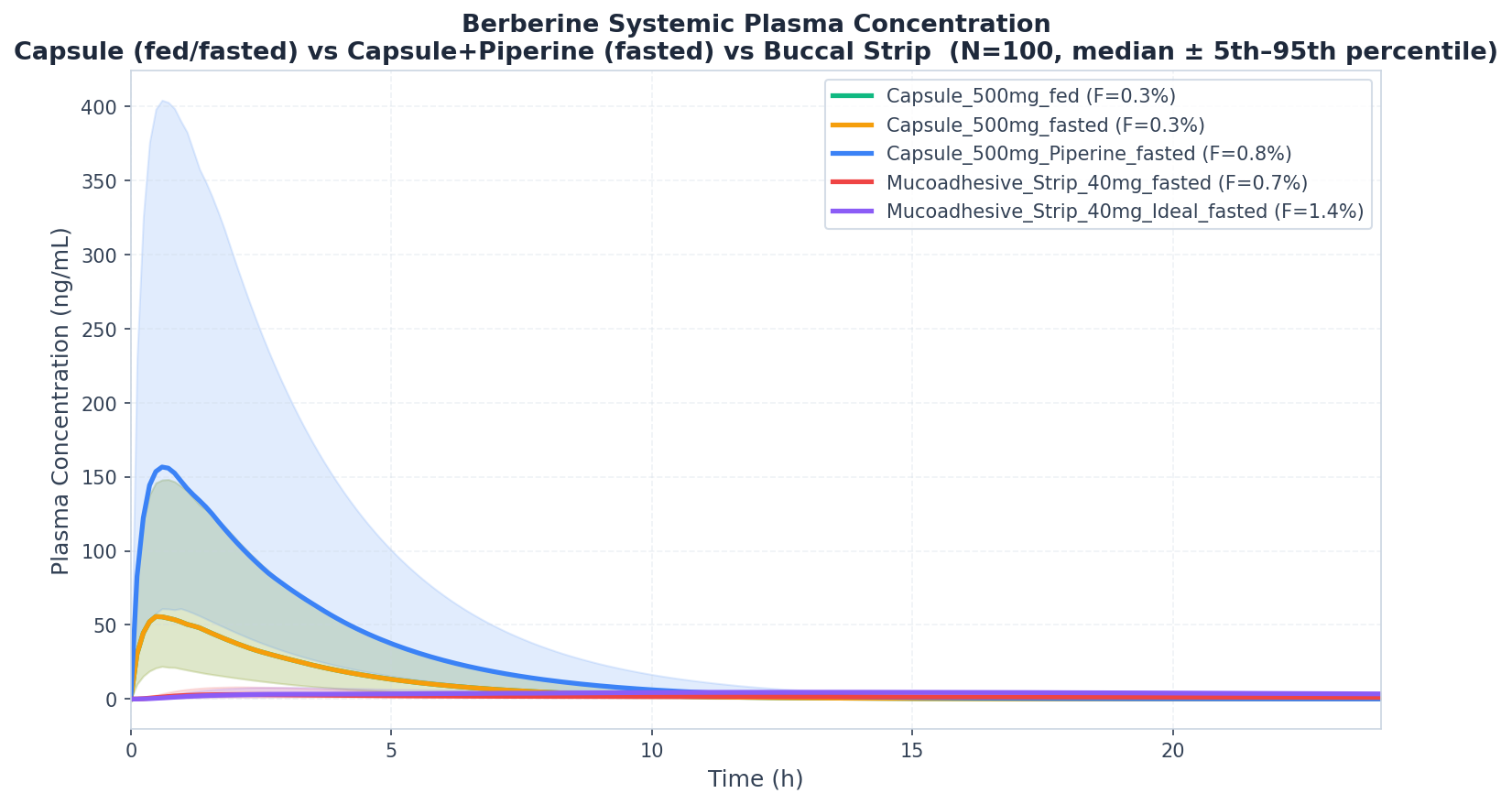
- Plasma Concentration–Time Profiles
- Median plasma concentration–time profiles (P5–P95 shaded), n=100.
Metabolic Fingerprint
CYP and UGT enzyme contributions to total intrinsic clearance, plus P-glycoprotein efflux substrate status. Values are derived from our GNN suite predictions and integrated into the PBPK simulation. The GNN models predict substrate probability, intrinsic clearance per enzyme, and inhibition probability — all applied during simulation.
Substrate Profile — Enzymes & Transporters
Intrinsic clearance (CLint) fractions per compound, predicted by our GNN suite from molecular structure. Bold teal = dominant clearance enzyme. These values are injected into the PBPK simulation to set per-enzyme gut-wall and hepatic clearance.
| Compound | CYP1A2 | CYP3A4 | CYP2D6 | CYP2C9 | CYP2C19 | UGT1A1 | SULT1A1 | P-gp Efflux |
|---|---|---|---|---|---|---|---|---|
| Berberine | — | 30.1% | 17.2% | 12.9% | — | 39.8% | — | Yes |
| Piperine | — | 26.3% | 15.8% | 12.3% | — | 45.6% | — | Yes |
- UGT1A1 glucuronidation is the dominant clearance pathway for both berberine (39.8%) and piperine (45.6%)
- CYP3A4 is the primary CYP pathway for berberine (30.1%) — piperine inhibits this enzyme, explaining the bioavailability boost
- Berberine P-gp substrate probability: 93% — strong efflux substrate; piperine inhibits P-gp, providing additional enhancement
- SULT1A1 contribution is 0% for both — sulfation is not a significant pathway for either compound
- Metabolic Insights
- Our GNN suite also predicts inhibition probabilities for each enzyme. These are used to compute cross-compound
DDI factors applied during simulation — piperine's inhibition of berberine's clearance enzymes is the mechanistic basis for the bioavailability enhancement.
Inhibition Profile — Enzymes & Transporters
| Compound | CYP1A2 | CYP3A4 | CYP2D6 | CYP2C9 | CYP2C19 | UGT1A1 | P-gp |
|---|---|---|---|---|---|---|---|
| Berberine | Yes | Yes | Yes | — | Yes | — | Yes |
| Piperine | Yes | Yes | — | — | Yes | — | Yes |
Piperine inhibits CYP3A4, CYP2D6, and CYP2C9 — the same enzymes responsible for berberine first-pass metabolism — as well as P-gp efflux. This cross-compound DDI is the mechanistic basis for the ~2.8× bioavailability boost observed in the piperine coadministration arm.