Simulaite Report
CBD / CBN Multi-Formulation Bioavailability Comparison
Pharmacokinetic Simulation — Gummies, Tinctures, and Oral Strips
April 22, 2026
Executive Summary
This report compares the oral bioavailability of CBD and CBN across 7 delivery formulations — buccal strips, sublingual strips, sublingual tincture, oral tincture, and gummies — at 25 mg dose per compound, using the Simulaite
PBPK engine on a virtual population of n=100 American individuals under both fasted and fed conditions. The simulation reveals dramatic differences between delivery routes — from <2% for swallowed formats (oral tincture, gummy) to >79% for ideal-patient buccal strips — driven by first-pass metabolism bypass, mucosal absorption kinetics, and food effects.
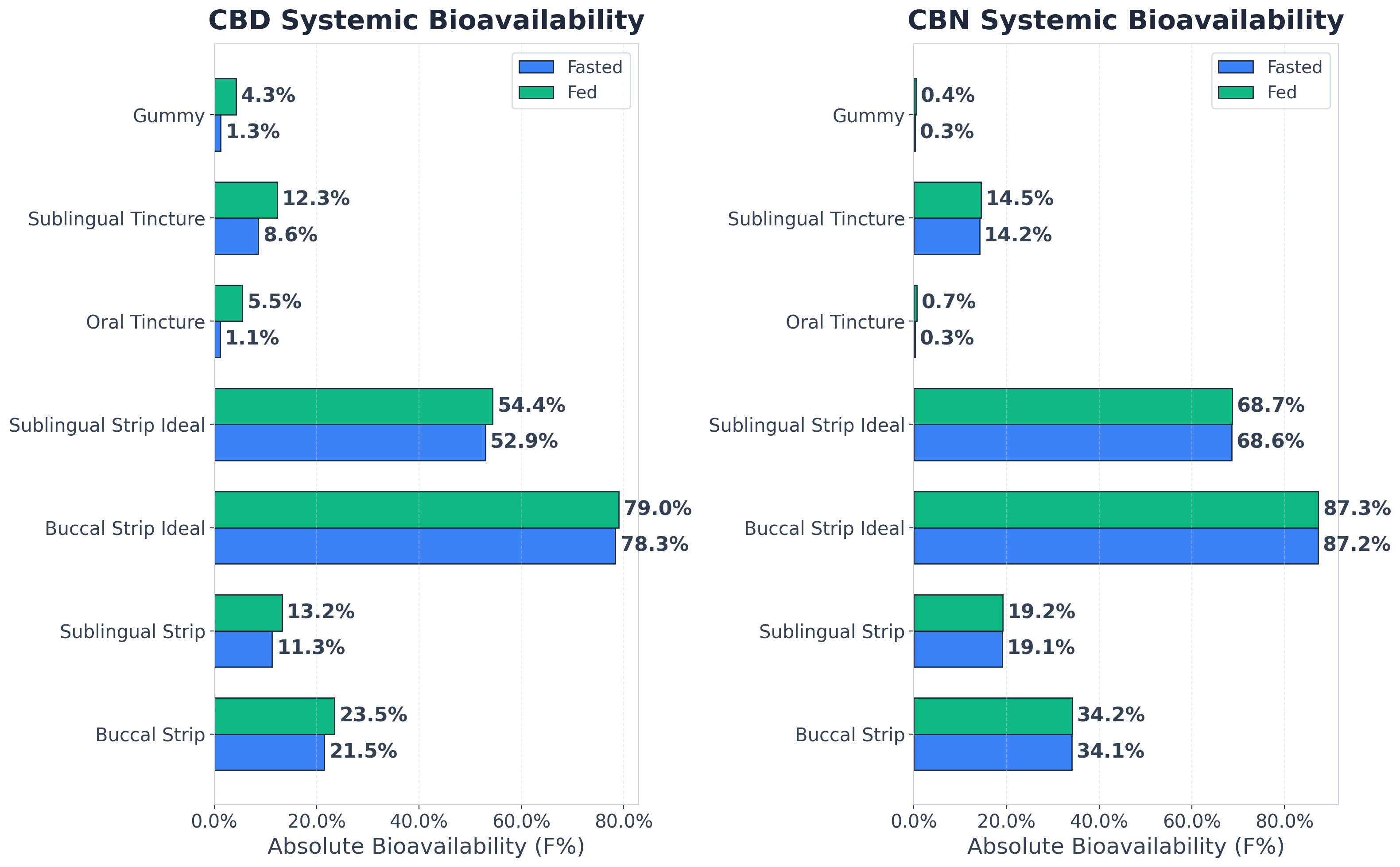
- Buccal strips achieve 22-78% CBD bioavailability (depending on patient swallowing) — significantly higher than oral formats
- Key Takeaways
- (gummy, tincture) which deliver <2% when administered non-sublingually and while fasted
- For transmucosal routes (buccal/sublingual), CBN outperforms CBD by 8-16% — but for swallowed routes, CBD actually does better than CBN (e.g., 1.3% vs 0.3% for gummy)
- Patients should minimize swallowing during strip dissolution — natural swallowing drops bioavailability about 4× (from 78% to 22%) as drug is lost to GI tract before full mucosal absorption
- Sublingual underperforms buccal by ~32-47% (depending on patient swallowing) — smaller surface area (10 vs 14 cm²) and higher salivary flow
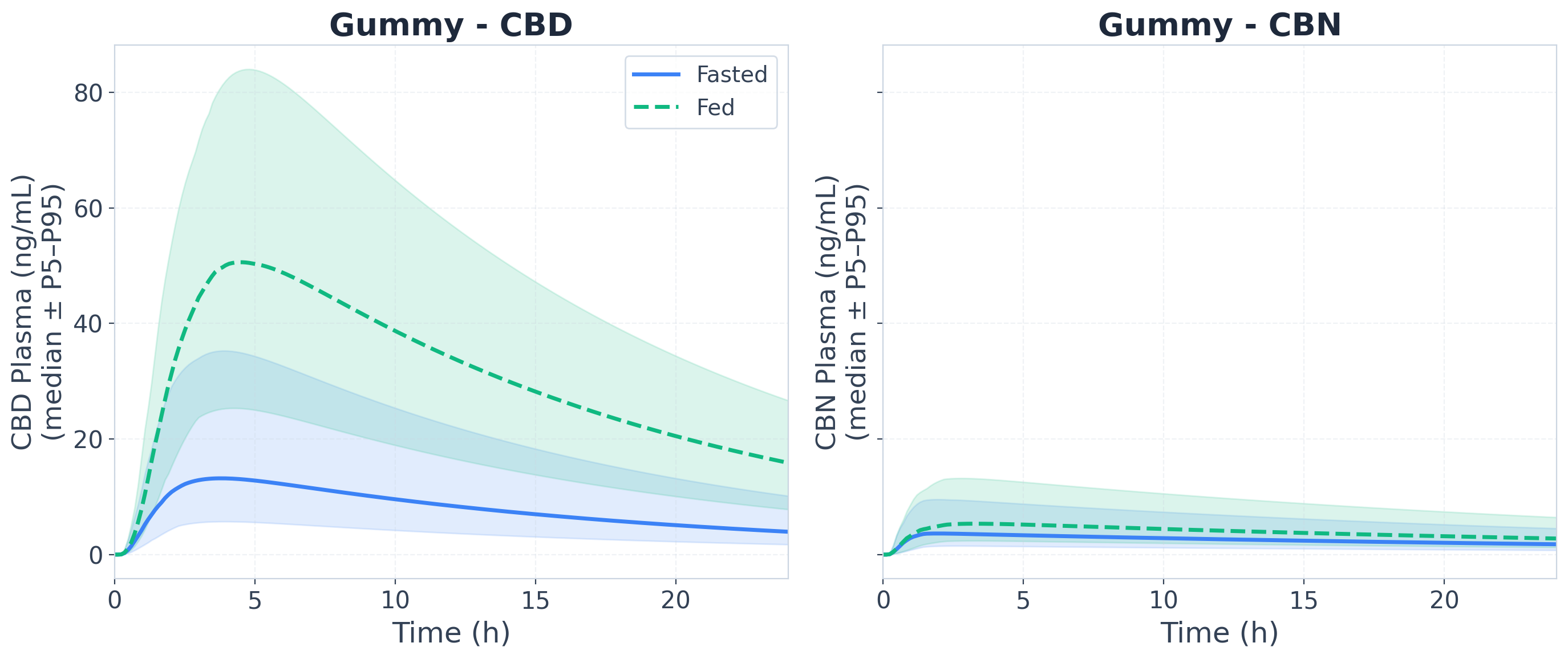
- Food intake dramatically boosts oral formats: 4.8× improvement for tincture (1.1% to 5.5% CBD) and 3.4× for gummy (1.3% to 4.3% CBD) — lipids stimulate lymphatic transport and slow GI transit
- Fed vs fasted makes little difference for transmucosal routes — absorption happens before swallowing, so first-pass bypass is already achieved
Molecule Profiles
| Name | SMILES | Formula |
|---|---|---|
| CBD (Cannabidiol) | CCCCCC1=CC(=C(C(=C1)O)[C@@H]2C=C(CC[C@H]2C(=C)C)C)O | C₂₁H₃₀O₂ |
| CBN (Cannabinol) | CCCCCC1=CC(=C2C(=C1)OC(C3=C2C=C(C=C3)C)(C)C)O | C₂₁H₂₆O₂ |
CBD and CBN are highly lipophilic phytocannabinoids derived from cannabis. Both compounds are significantly metabolized by CYP and UGT enzymes warranting transmucosal delivery to bypass first-pass metabolism. Their lipophilicity enables lymphatic transport with specialized delivery systems and/or having a fat-heavy meal while taking them. We use our suite of graph neural networks to predict relevant molecular properties and interactions with liver enzymes, plasma proteins, and the gut wall to inform the simulations.
Formulation Parameters
1. Buccal Strip
- Delivery Type
- Oral Fast-Dissolving Strip
- Route
- Buccal (cheek)
- Surface Area
- 3.5 × 4 cm (14 cm²)
- Dissolve Time
- ~30 min
- Dose per Compound
- 25 mg
- Lipid Excipient
- None (polymer matrix)
- Patient Type
- Standard (includes natural swallowing)
2. Sublingual Strip
- Delivery Type
- Oral Fast-Dissolving Strip
- Route
- Sublingual (under tongue)
- Surface Area
- 2.5 × 4 cm (10 cm²)
- Dissolve Time
- ~20 min
- Dose per Compound
- 25 mg
- Lipid Excipient
- None (polymer matrix)
- Patient Type
- Standard (includes natural swallowing)
3. Buccal Strip — Ideal Patient
- Delivery Type
- Oral Fast-Dissolving Strip
- Route
- Buccal (cheek)
- Surface Area
- 3.5 × 4 cm (14 cm²)
- Dissolve Time
- ~30 min
- Dose per Compound
- 25 mg
- Lipid Excipient
- None (polymer matrix)
- Patient Type
- Ideal (refrains from swallowing)
4. Sublingual Strip — Ideal Patient
- Delivery Type
- Oral Fast-Dissolving Strip
- Route
- Sublingual (under tongue)
- Surface Area
- 2.5 × 4 cm (10 cm²)
- Dissolve Time
- ~20 min
- Dose per Compound
- 25 mg
- Lipid Excipient
- None (polymer matrix)
- Patient Type
- Ideal (refrains from swallowing)
5. Oral MCT Tincture
- Delivery Type
- Liquid Tincture
- Route
- Oral (swallowed)
- Volume
- 1 mL
- Dose per Compound
- 25 mg
- Lipid Excipient
- MCT Oil
- Administration
- Swallowed immediately
6. Sublingual MCT Tincture
- Delivery Type
- Liquid Tincture
- Route
- Sublingual hold then swallow
- Volume
- 1 mL
- Dose per Compound
- 25 mg
- Lipid Excipient
- MCT Oil
- Hold Time
- 1.5 min (90 sec)
7. MCT + Lecithin Gummy
- Delivery Type
- Solid Gummy
- Route
- Oral (swallowed)
- Weight
- ~3 g
- Dose per Compound
- 25 mg
- Lipid Excipient
- MCT Oil + Lecithin
- Release Profile
- Gradual release over ~45 min
Population Settings
A virtual population of 100 American individuals was generated using population physiology from pharmaceutical databases. Each individual has unique organ volumes, blood flows, and enzyme expression levels derived from clinical datasets, capturing inter-individual variability in absorption, distribution, and clearance. Both fasted and fed states were simulated to assess the impact of food on bioavailability.
| Parameter | Value |
|---|---|
| Sample Size (n) | 100 |
| Sex | 49% female, 51% male |
| Age Range | 18.0–64.2 years (mean 40.5) |
| Body Weight | 47.3–133.4 kg (mean 78.7) |
| BMI Range | 17.4–45.7 (mean 27.7) |
| Ethnicity | White 62% · Latino 19% · African American 13% · Asian 6% |
| Prandial States | Fasted & Fed (both simulated) |
Bioavailability Results
- Bioavailability (F%) Comparison
- Absolute bioavailability (F%) for each formulation under fasted and fed conditions, computed as: F% = AUC(oral or transmucosal) / AUC(IV bolus)
× 100. The IV bolus serves as the 100% reference — it bypasses all absorption barriers and delivers drug directly to systemic circulation.
- AUC (ng/mL·h) — Fasted State
- AUC captures the clinically relevant inter-individual variability — driven by differences in clearance, volume of distribution, and (for oral routes) GI
absorption. CV% reflects real patient-to-patient exposure differences.
| Formulation | CBD AUC (mean±SD) | CBD CV% | CBN AUC (mean±SD) | CBN CV% |
|---|---|---|---|---|
| Buccal Strip | 3980 ± 842 | 21% | 8780 ± 1874 | 21% |
| Sublingual Strip | 2093 ± 436 | 21% | 4917 ± 1046 | 21% |
| Buccal Strip — Ideal | 14517 ± 3122 | 22% | 22466 ± 4806 | 21% |
| Sublingual Strip — Ideal | 9809 ± 2102 | 21% | 17666 ± 3777 | 21% |
| Oral Tincture | 204 ± 114 | 56% | 64 ± 36 | 56% |
| Sublingual Tincture | 1589 ± 529 | 33% | 3668 ± 1266 | 35% |
| Gummy | 227 ± 126 | 56% | 73 ± 40 | 55% |
Absorption Pathway Breakdown — Transmucosal Formulations (Fasted)
In standard patients, natural swallowing during strip dissolution significantly increases the swallowed fraction (drug lost to GI tract before full mucosal absorption). In ideal patients, only passive salivary flow contributes to swallowing, resulting in minimal loss.
| Formulation | CBD Absorbed % | CBD Swallowed % | CBN Absorbed % | CBN Swallowed % |
|---|---|---|---|---|
| Buccal Strip | 60.0% | 40.0% | 68.7% | 31.3% |
| Sublingual Strip | 45.0% | 55.0% | 51.4% | 48.6% |
| Buccal Strip — Ideal | 94.3% | 5.7% | 96.2% | 3.8% |
| Sublingual Strip — Ideal | 84.4% | 15.6% | 88.0% | 12.0% |
Absorbed = drug reaching systemic circulation via oral mucosa (bypasses first-pass). Swallowed = drug lost to GI tract before mucosal absorption.
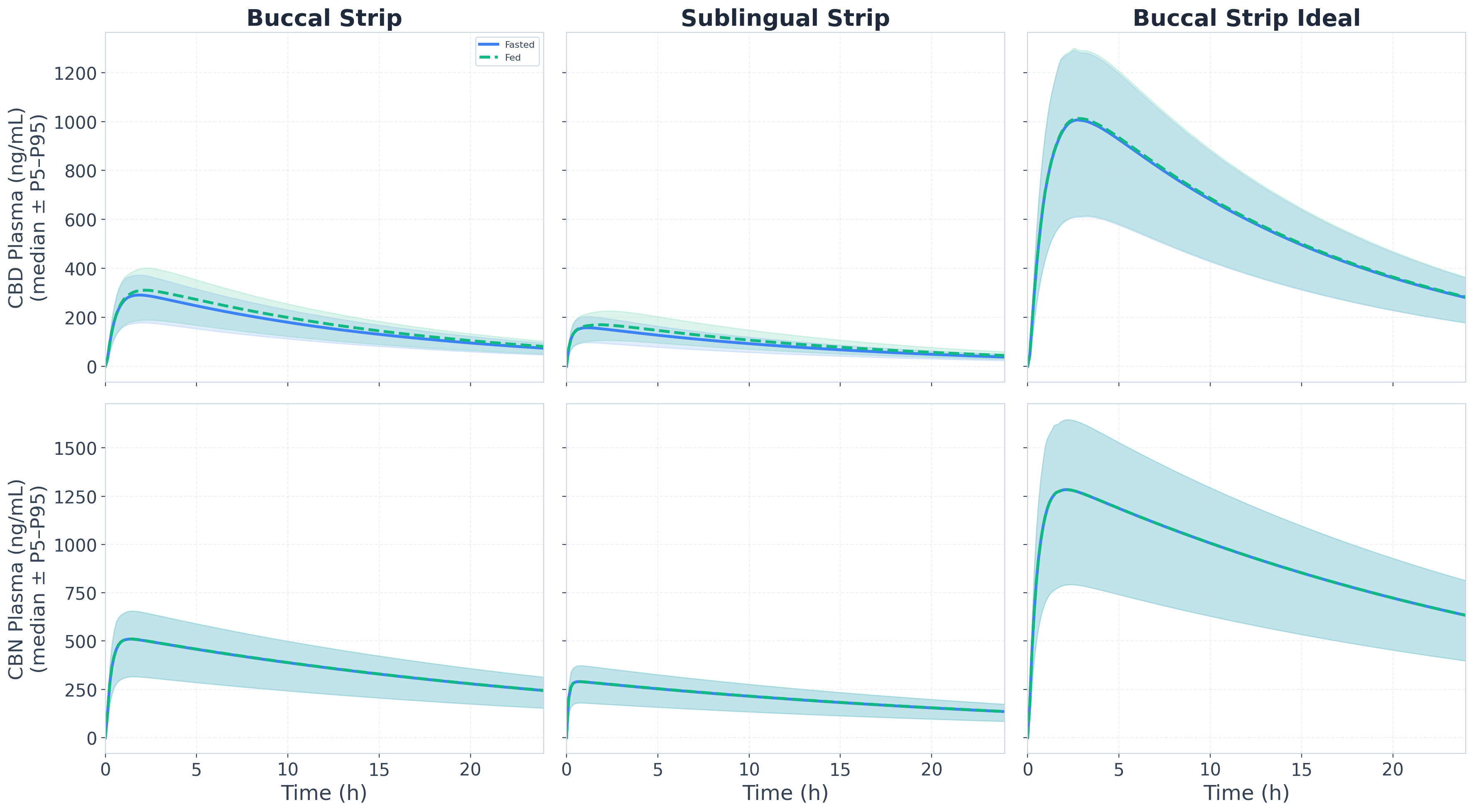
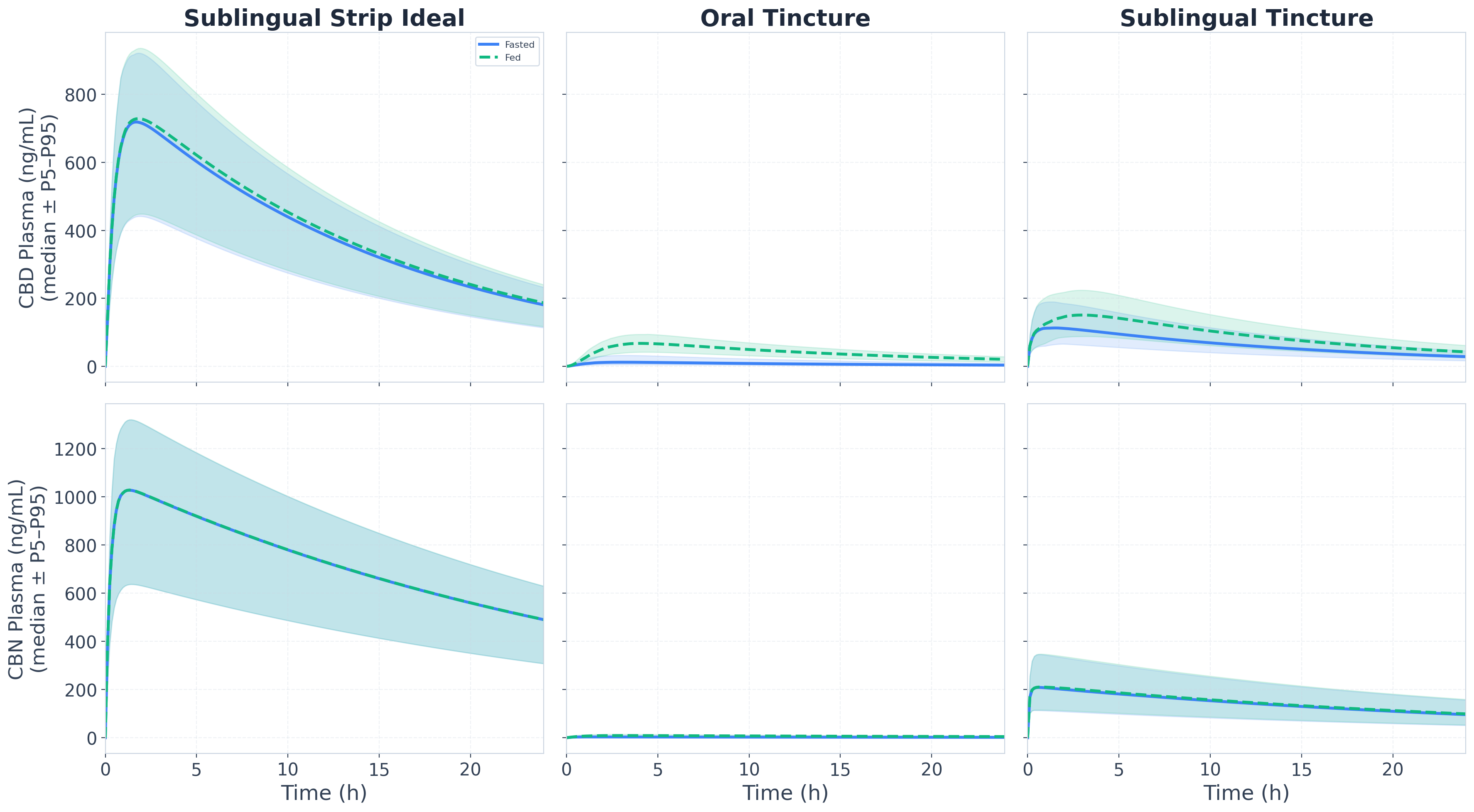
- Plasma Concentration–Time Profiles
- Median plasma concentration–time profiles (P5–P95 shaded), fasted (solid) and fed (dashed), n=100.
Metabolic Fingerprint
CYP and UGT enzyme contributions to total intrinsic clearance, plus P-glycoprotein efflux substrate status. Values are compound properties derived from GNN predictions and integrated into the PBPK simulation. Substrate and inhibition magnitude is applied during simulation (not shown).
Substrate Profile — Enzymes & Transporters
Intrinsic clearance (CLint) fractions per compound. Bold teal = dominant clearance enzyme.
| Compound | CYP1A2 | CYP3A4 | CYP2D6 | CYP2C9 | CYP2C19 | UGT1A1 | SULT1A1 | P-gp Efflux |
|---|---|---|---|---|---|---|---|---|
| CBD | 0.0% | 28.3% | 18.8% | 11.5% | 0.0% | 41.4% | 0.0% | Yes |
| CBN | 0.0% | 26.8% | 17.2% | 12.4% | 0.0% | 43.6% | 0.0% | Yes |
- UGT1A1 glucuronidation is the dominant clearance pathway for both CBD (41.4%) and CBN (43.6%) — consistent with extensive Phase II conjugation of cannabinoids.
- CYP3A4 is the dominant CYP pathway for both (CBD: 28.3%, CBN: 26.8%). CYP2D6 is a consistent secondary pathway
Metabolic Insights
(CBD: 18.8%, CBN: 17.2%).
- SULT1A1 contribution is 0% for both compounds — sulfation is not a significant pathway for cannabinoids at these doses.
GNN predictions for enzyme inhibition. Inhibition magnitude is also predicted by our GNN suite and applied during simulation (not shown). CBD inhibits CYP3A4 and CYP2C9; CBN inhibits a broader panel including CYP1A2, CYP3A4, CYP2D6, CYP2C9, and CYP2C19. MCT Oil (excipient in tincture/gummy formulations) provides additional CYP3A4 inhibition at gut-wall concentrations.
Inhibition Profile — Enzymes & Transporters
| Component | CYP1A2 | CYP3A4 | CYP2D6 | CYP2C9 | CYP2C19 | UGT1A1 | SULT1A1 | P-gp |
|---|---|---|---|---|---|---|---|---|
| CBD | — | Yes | — | Yes | — | — | — | — |
| CBN | Yes | Yes | Yes | Yes | Yes | — | — | — |
| MCT Oil (C8 FFA) (excipient) | — | Yes | — | — | — | — | — | — |
Both CBD and CBN inhibit CYP3A4 and CYP2C9 — clinically relevant for co-administration with statins, warfarin, immunosuppressants, and other CYP3A4/2C9 substrates. CBN additionally inhibits CYP1A2, CYP2D6, and CYP2C19 with high probability, giving it a broader DDI risk profile.
Clinical Literature Comparison
Our simulation results are contextualized against published clinical studies examining CBD bioavailability across different delivery routes and prandial states.
1. CURE Pharmaceutical OTF Study (2022)
Source: CURE Pharmaceutical OTF Study — worldpharmatoday.com/news/cure-pharmaceutical-cbd-oral-thin-film- pharmacokinetic-study-shows-improved-bioavailability-compared-to-cbd-soft-gel/. CBD Oral Thin Film (OTF) pharmacokinetic study. CUREform™ delivery platform (solubilization + encapsulation). 25 mg CBD OTF vs 25 mg CBD soft gel in 14 healthy adults.
- Relevance
- Our buccal/sublingual strip delivery is mechanistically similar to OTF (oral transmucosal). Both show improved bioavailability
vs swallowed formulations. The CURE study confirms that transmucosal delivery of CBD achieves significantly higher Cmax and faster Tmax than soft gel — consistent with our simulation showing 21.5% F for buccal strip vs 1.1% for oral tincture.
2. Della Rocca et al. (2022) — Oral vs OTM in Dogs
Source: Della Rocca et al. (2022) — https://doi.org/10.3389/fvets.2022.1104152 CBD 1 mg/kg oral vs oral transmucosal (OTM) in 12 dogs. Result: Cmax ~207 ng/mL (oral) vs ~200 ng/mL (OTM), Tmax ~2.2h vs ~1.9h — no significant difference.
Relevance to Our Simulation
- The dog study found no OTM benefit — consistent with our simulation showing that when swallowing is not controlled, sublingual bioavailability approaches oral levels.
3. Saals et al. (2025) — High-Fat Meal Effect
Source: Saals et al. (2025) — https://doi.org/10.1038/s41598-025-87621-4 Single oral dose CBD-rich extract (70 mg CBD equivalent). High-fat meal vs fasting in 11 healthy participants. Fed/Fasted Cmax ratio: 17.4× (90% CI 12.4–24.2). Fed/Fasted
AUC ratio: 9.7× (90% CI 7.7–12.3).
Comparison to Our Simulation
- Our PBPK simulation shows a 4.8× fed/fasted ratio for CBD oral tincture and 3.4× for gummy — similar magnitude to the 9.7× AUC increase observed clinically (capsule format).
- The clinical study used a high-fat meal (55-65g fat) while our simulation uses 30g fat. Despite this difference, both show substantial fed-state enhancement, demonstrating the powerful effect of fat on cannabinoid bioavailability.
- The fed-state enhancement is driven by lymphatic transport and increased bile salt solubilization — mechanisms captured in our PBPK model.